|
Overview
 Fallen arches, the medical term for flat feet, are simply feet that do not arch in the middle. Such feet lay flat with the whole of the sole on the ground. All children are born with flat feet, but as they grow the feet normally develop an arch so that by the age of ten almost all children have arched feet. Occasionally a child will not develop properly arched feet. This may be due to a bone malformation present at birth, or abnormalities in ligaments within the feet or legs that cause the child's weight to be unevenly distributed. Causes Footwear: shoes which limit toe movement; high heels. Barefoot walking may be protective. A tight Achilles tendon or calf muscles (heel cord contracture). This may help to cause Pes Planus, or may contribute to symptoms such as foot pain when there is existing Pes Planus. Obesity. Other bony abnormalities, eg rotational deformities, tibial abnormalities, coalition (fusion) of tarsal bones, equinus deformity. Ligamentous laxity, eg familial, Marfan's syndrome, Ehlers-Danlos syndrome, Down's syndrome. Other factors causing foot pronation, eg hip abductor weakness and genu valgum. Symptoms Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle. Diagnosis Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis. arch support inserts reviews Non Surgical Treatment In many cases of PTTD, treatment can begin with non-surgical approaches that may include orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support. Surgical Treatment  In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you. Overview
Having one leg shorter than the other is a common physical condition. It has two primary causes--structural or functional problems. Structural differences in length can be the result of growth defect, previous injuries or surgeries. Functional differences in length can result from altered mechanics of the feet, knee, hip and/or pelvis. These altered mechanics from functional leg length discrepancy often stem from having an unbalanced foundation.  Causes From an anatomical stand point, the LLD could have been from hereditary, broken bones, diseases and joint replacements. Functional LLD can be from over pronating, knee deformities, tight calves and hamstrings, weak IT band, curvature in the spine and many other such muscular/skeletal issues. Symptoms Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities. Diagnosis Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue. Non Surgical Treatment Non-surgical treatment can be effective. A shoe lift may be recommended if the leg length difference is less than 1 inch. More significant leg length discrepancies may require a surgical procedure. In children, surgical procedures are available to help make leg lengths more equal.  how to increase height after 25 Surgical Treatment Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age. Overview
 Heel pain is a common foot condition. It's usually felt as an intense pain when using the affected heel. Heel pain usually builds up gradually and gets worse over time. The pain is often severe and occurs when you place weight on the heel. In most cases, only one heel is affected, although estimates suggest that around a third of people have pain in both heels. The pain is usually worse first thing in the morning, or when you first take a step after a period of inactivity. Walking usually improves the pain, but it often gets worse again after walking or standing for a long time. Some people may limp or develop an abnormal walking style as they try to avoid placing weight on the affected heel. Causes A flattening or overstretching of your plantar fascia can cause microscopic tears, inflammation, and a burning sensation. While developing slowly, there may be a sudden severe event sometimes occurring in only one foot at a time. Plantar Faciitis can affect people of all ages and backgrounds. Some contributing factors include age, weight-bearing activities, sudden increase in physical activity, improper shoes, excess weight or a recent weight gain (as little as 5 pounds), and poor biomechanics (flat feet, high arches or unnatural gait). Symptoms Plantar fasciitis is a condition of irritation to the plantar fascia, the thick ligament on the bottom of your foot. It classically causes pain and stiffness on the bottom of your heel and feels worse in the morning with the first steps out of bed and also in the beginning of an activity after a period of rest. For instance, after driving a car, people feel pain when they first get out, or runners will feel discomfort for the first few minutes of their run. This occurs because the plantar fascia is not well supplied by blood, which makes this condition slow in healing, and a certain amount of activity is needed to get the area to warm up. Plantar fasciitis can occur for various reasons: use of improper, non-supportive shoes; over-training in sports; lack of flexibility; weight gain; prolonged standing; and, interestingly, prolonged bed rest. Diagnosis A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem. Non Surgical Treatment Physical medicine modalities are well known for their benefits and they have been consistently applied in early treatment of plantar fasciitis. Typically, the direct application of ice, ice baths or contrast soaking aid in the local reduction of inflammation and temporarily augment pain management. Electric stimulation may only provide indirect reduction of interstitial inflammation of the plantar fascia. Ultrasound therapy, hot pack systems and deep tissue massage help eliminate inflammation and aid in restoring plantar fascia tensegrity. Generally, these modalities are considered to be valuable adjuncts to a well-organised treatment plan. Various programs of stretching, range of motion and therapeutic exercises can help re-establish foot function and improve tolerance to load. When it is done appropriately, stretching can serve as an important adjunct to the resumption of the plantar fascia?s ability to tolerate eccentric loading forces that typically occur during stance and gait. Night splinting has proven to be an effective tool in managing persistent plantar fasciitis. Antiinflammatory modalities, such as ice and ice baths, are often the first line of treatment. Oral NSAIDs have been a mainstay of treatment. While they effectively relieve symptoms, be aware that they frequently fail to promote sustained relief. When inflammation is severe or fails to respond to initial efforts, one may consider corticosteroid injection(s). However, keep in mind that corticosteroid injections impose the risk of aponeurosis rupture secondary to focal collagen tissue necrosis and can result in focal heel fat pad atrophy. Surgical Treatment With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick. back of heel cushions Prevention  Wearing real good, supportive shoes are a great way to avoid heel pain. Usually, New Balance is a good shoe to wear, just for everyday shoe gear. By wearing proper footwear and performing thorough stretches, athletes can help prevent frequent heel pain. If you are starting to get a little discomfort or pain in the feet or heel, know that pain is not normal. So if you are having pain, you should be proactive and visit our office. If you let heel pain get out of control you could run into several other problems. It is always suggested to visit a podiatrist whenever you are experiencing pain. Overview
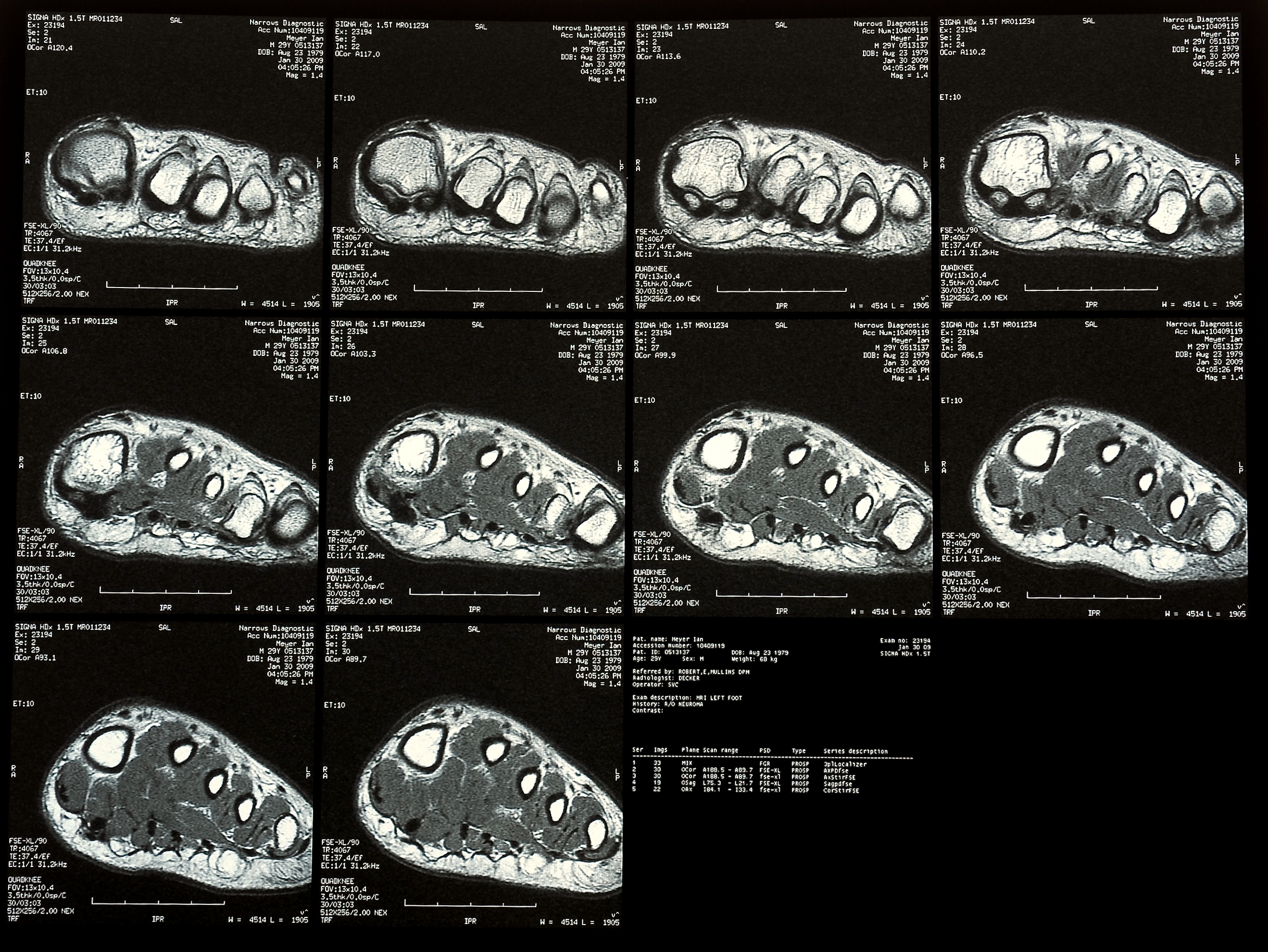 Morton?s Neuroma is a common foot condition characterized by pain and swelling in the ball of the foot, between the third and fourth toes. It?s caused by bones in your feet squeezing a nerve. Symptoms include a sharp, burning pain and possibly separation between the affected toes. Morton?s Neuroma is a common foot condition characterized by pain and swelling in the ball of the foot, between the third and fourth toes. It?s caused by bones in your feet squeezing a nerve. Symptoms include a sharp, burning pain and possibly separation between the affected toes.Causes There are many reasons to develop a neuroma. Improper shoe gear is probably the most likely cause. Repetitive activity and excessive pressure on the ball of the foot are common. Heredity and genetic factors may also be involved. In many cases the structure of the foot may predispose the condition. Associated conditions that may cause neuroma include: bunion, hammer toes, ligament laxity, and/or a tight calf muscle. Some patients may have thinning of the fat pad on the ball of the foot, which may result in increased pressure of the nerves. Tight pointy shoes (and high heels) without padding may induce pain in the ball of the foot. Neuroma may occur suddenly, or develop over time. Symptoms Patients will feel pain that worsens with walking, particularly when walking in shoes with thin soles or high heels. Also, anything that squeezes the metatarsal heads together may aggravate symptoms, such as narrow shoes. A patient may feel the need to remove the shoe and rub the foot to soothe the pain. Diagnosis Morton?s neuroma can be identified during a physical exam, after pressing on the bottom of the foot. This maneuver usually reproduces the patient?s pain. MRI and ultrasound are imaging studiesthat can demonstrate the presence of the neuroma. An x-ray may also be ordered to make sure no other issues exist in the foot. A local anesthetic injection along the neuroma may temporarily abolish the pain, and help confirm the diagnosis. Non Surgical Treatment Wearing shoes that provide enough room in the toe box is also the first step in treating Morton?s neuroma. For instant relief when pain flares up, try taking your shoes off and rubbing the area. The nerve can get trapped below the ligament, and rubbing can move it back to its natural position. Your doctor or a foot-care specialist may recommend lower heels and metatarsal pads. These pads provide cushioning under your neuroma and better arch support to redistribute your weight. If you keep pressure off the toes and wear wide enough shoes, the problem may gradually disappear.  Surgical Treatment For severe or persistent pain, you may need surgery to remove the neuroma. Once the nerve is gone, you permanently lose feeling in the affected area. One alternative to surgery is to undergo neurolysis injections. These use chemical agents to block pain signals. Another alternative is to take a prescription pain reliever that alleviates nerve pain. There are actually not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital implies that you are born with it. One leg is anatomically shorter than the other. Through developmental periods of aging, the brain senses the walking pattern and identifies some variation. The body typically adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch isn't really uncommon, require Shoe Lifts to compensate and normally won't have a serious effect over a lifetime.
 Leg length inequality goes typically undiscovered on a daily basis, however this condition is easily fixed, and can eliminate a number of cases of back discomfort. Treatment for leg length inequality typically involves Shoe Lifts. These are generally very inexpensive, commonly costing under twenty dollars, compared to a custom orthotic of $200 and up. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Back pain is the most widespread ailment affecting men and women today. Over 80 million men and women are afflicted by back pain at some stage in their life. It is a problem that costs businesses millions annually due to time lost and production. Fresh and improved treatment solutions are constantly sought after in the hope of minimizing the economic influence this issue causes.  People from all corners of the earth experience foot ache as a result of leg length discrepancy. In a lot of these cases Shoe Lifts might be of very useful. The lifts are capable of reducing any discomfort and pain in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic physicians. In order to support the human body in a balanced manner, feet have a crucial part to play. Despite that, it's often the most neglected area in the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This will cause other areas of the body like knees, ankles and backs to be impacted too. Shoe Lifts guarantee that the right posture and balance are restored. There are actually not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental stages of aging, the human brain picks up on the gait pattern and identifies some variance. Your body typically adapts by tilting one shoulder to the "short" side. A difference of less than a quarter inch isn't grossly irregular, does not need Shoe Lifts to compensate and mostly doesn't have a serious effect over a lifetime.
 Leg length inequality goes typically undiagnosed on a daily basis, yet this issue is simply corrected, and can eradicate a number of instances of chronic back pain. Therapy for leg length inequality usually consists of Shoe Lifts. Many are very inexpensive, usually priced at less than twenty dollars, compared to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position. Chronic back pain is the most common ailment afflicting men and women today. Over 80 million men and women experience back pain at some point in their life. It is a problem which costs employers vast amounts of money yearly because of time lost and production. Innovative and improved treatment methods are constantly sought after in the hope of reducing the economic impact this condition causes.  People from all corners of the earth experience foot ache as a result of leg length discrepancy. In these types of situations Shoe Lifts can be of immense help. The lifts are capable of decreasing any pain in the feet. Shoe Lifts are recommended by numerous qualified orthopaedic orthopedists. In order to support the human body in a healthy and balanced manner, your feet have a very important part to play. Irrespective of that, it is sometimes the most overlooked area of the body. Many people have flat-feet which means there is unequal force exerted on the feet. This causes other areas of the body including knees, ankles and backs to be impacted too. Shoe Lifts ensure that ideal posture and balance are restored. There are not one but two different types of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter than the other. As a result of developmental periods of aging, the brain picks up on the walking pattern and recognizes some variance. The body usually adapts by tilting one shoulder over to the "short" side. A difference of less than a quarter inch is not really uncommon, doesn't need Shoe Lifts to compensate and typically doesn't have a serious effect over a lifetime.
 Leg length inequality goes typically undiscovered on a daily basis, yet this condition is simply corrected, and can eradicate a number of incidents of upper back pain. Therapy for leg length inequality commonly consists of Shoe Lifts. These are very reasonably priced, frequently being below twenty dollars, in comparison to a custom orthotic of $200 and up. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Lower back pain is easily the most prevalent health problem afflicting men and women today. Over 80 million men and women are afflicted by back pain at some point in their life. It is a problem that costs employers huge amounts of money yearly because of lost time and production. New and improved treatment methods are continually sought after in the hope of lowering economic impact this issue causes.  People from all corners of the world suffer from foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts are usually of immense help. The lifts are capable of relieving any pain and discomfort in the feet. Shoe Lifts are recommended by countless specialist orthopaedic physicians. So that they can support the body in a well-balanced manner, the feet have got a crucial part to play. Irrespective of that, it can be the most overlooked zone of the body. Many people have flat-feet meaning there is unequal force placed on the feet. This causes other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts ensure that suitable posture and balance are restored.
Overview
Arch pain occurs with an inflammation of the plantar arch or fascia. It is the thick membrane that covers and supports all the muscles of the sole of the foot from the heel bone to the base of the toes that is called plantar arch. When this membrane pulls excessively (constant strain), pain developes in the arch of the foot or heel.  Causes Recent research has found a link with changes to the tendon in the foot and an increase in a type of protein called proteolytic enzyme. These enzymes can break down some areas of the tendon, weakening it and causing the foot arch to fall. Similar changes are also seen in other conditions, such as Achilles tendonitis. This could have important implications for treating flat feet because medication that specifically targets these enzymes could provide an alternative to surgery. However, further research is needed and this type of treatment is thought to be about 10 to 15 years away. Symptoms Flat feet don't usually cause problems, but they can put a strain on your muscles and ligaments (ligaments link two bones together at a joint). This may cause pain in your legs when you walk. If you have flat feet, you may experience pain in any of the following areas, the inside of your ankle, the arch of your foot, the outer side of your foot, the calf, the knee, hip or back, Some people with flat feet find that their weight is distributed unevenly, particularly if their foot rolls inwards too much (overpronates). If your foot overpronates, your shoes are likely to wear out quickly. Overpronation can also damage your ankle joint and Achilles tendon (the large tendon at the back of your ankle). See your GP if you or your child has flat feet and your feet are painful, even when wearing supportive, well-fitting shoes, shoes wear out very quickly, feet appear to be getting flatter, feet are weak, numb or stiff, Your GP may refer you to a podiatrist (foot specialist). Diagnosis The diagnosis of high arch (cavus) foot deformity or Charcot Marie Tooth disease can be made by an orthopedic surgeon in the office. Evaluation includes a thorough history and physical examination as well as imaging studies such as X-rays. The orthopedic surgeon will look at the overall shape, flexibility, and strength of a patient?s foot and ankle to help determine the best treatment. Nerve tests may occasionally need to be performed to help confirm the diagnosis. Non Surgical Treatment For mild pain or aching, acetaminophen (Tylenol) or a nonsteroidal anti-inflammatory drug (NSAID), such as aspirin or ibuprofen (Advil, Motrin and others) may be effective. When there are no symptoms, treatment is not needed. If a child older than age 3 develops symptoms, the doctor may prescribe a therapeutic shoe insert made from a mold of the child's foot or a corrective shoe. As an alternative, some doctors recommend store-bought arch supports. These appear to work as well as more expensive treatments in many children. With any conservative, nonsurgical treatment, the goal is to relieve pain by supporting the arch and correcting any imbalance in the mechanics of the foot. Surgery is typically offered as a last resort in people with significant pain that is resistant to other therapies.  Surgical Treatment In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. Stretching Exercises Calf Raises. Strengthens the tendons in your heels and calf muscles, which support your arch. Raise up on the balls of your feet as high as possible. Slowly lower down. Do three sets of 10 reps. Progress to doing the raises on stairs (with heels hanging off), and then to single-leg raises. Step Stretch. Improves flexibility in your Achilles tendon and calf-when these areas become tight, the arch gets painfully overloaded. Stand at the edge of a step, toes on step, heels hanging off. Lower your heels down, past the step, then raise back up to the start position. Do three sets of 10 reps. Doming. Works the arch muscles and the tibialis posterior (in the calf and foot) to control excess pronation. While standing, press your toes downward into the ground while keeping the heel planted, so that your foot forms an arch (or dome). Release, and do three sets of 10 reps on each foot. Toe Spread and Squeeze. Targets the interossei muscles of the foot, which support the arch. While sitting, loop a small resistance band around your toes. Spread toes; release. Then place a toe separator (used at nail salons) in between toes. Squeeze toes in; release. Do three sets of 10 reps of each exercise on both feet. Towel Curls. Works the toe-flexor muscles that run along your arch to increase overall foot strength. Lay a small hand towel on the floor, and place one foot on the towel. Using just your toes, scrunch the towel toward you, hold, then slowly push the towel away from you back to start position. Do three sets of 10 reps on each foot.
Overview
You arch is the curved, raised area made up of your tarsal and metatarsal bones. It helps distribute some of your body weight off of your heel. It is shaped slightly different for everyone-some have lower or ?flatter? arches than others. This doesn?t always cause pain, but when it does, it can make walking and standing unpleasant and difficult. Generally the muscles and other tissues along the arch and even in the heel ache. The inside of the foot and ankle can also swell uncomfortably. Sometimes arches ?fall? inward from an injury or weakness, flattening out an otherwise normal foot.  Causes If the feet are exposed to damp conditions for prolonged periods, you can develop Trench Foot. Most commonly associated with World War One, it now tends to be seen in builders, hikers or festival goers. Trench foot causing numbness and bottom of foot pain. With Trench Foot, the sole of the foot turns a white/grey colour and you may develop pins and needles or numbness. Other symptoms include pain in bottom of foot and swelling. If left untreated, you can develop blisters and permanent nerve damage which can lead to the need for amputation. Treatment and prevention aim to reduce the dampness around the foot and ensure good foot hygiene. Slowly rewarming the feet and using special products in a foot bath really helps reduce the damage and foot arch pain from Trench Foot. Symptoms Repetitive exertive activity arch pain is usually sharp, and localized to a specific area, rather than the entire arch. Usually the pain occurs in the area just in front of the heel. It is present when first standing on the foot in the morning, but may decrease once you start walking around, but will, gradually becomes worse with continued walking or running. Swelling may be present. The pain subsides with rest, but stretching the arch while resting may cause the pain to return. Injury pain is constantly present, but worse when standing on the foot. This pain is localized to a specific area, but may radiate out from this area to the entire foot. The pain is sharp, and usually accompanied by swelling and occasionally "black and blue" discolorations. The pain due to the natural aging process is usually dull and aching, or stiff, and can be felt throughout the entire arch area, rather then in just one spot. This pain is present whenever weight bearing, and usually becomes worse with continued walking. The pain gradually subsides when resting, and usually does not return with stretching. Biomechanical defect pain is usually localized to a section of the arch, such as the inner, middle, outer, front, or back of the arch. This pain may be sharp or dull, but is always worse with continued walking. Diagnosis Flat feet are easy to identify while standing or walking. When someone with flat feet stands, their inner foot or arch flattens and their foot may roll over to the inner side. This is known as overpronation. To see whether your foot overpronates, stand on tiptoes or push your big toe back as far as possible. If the arch of your foot doesn't appear, your foot is likely to overpronate when you walk or run. It can be difficult to tell whether a child has flat feet because their arches may not fully develop until they're 10 years of age. Non Surgical Treatment Just as there are many different causes of flat feet, there are also many different treatment options. The most important aspect of treatment is determining the exact type or underlying cause of flat feet that you have. Foot and ankle specialists can determine this through thorough clinical examination and special imaging studies (e.g., x-rays, computed tomography, and/or magnetic resonance imaging). Conservative treatment is effective in the vast majority of flat foot cases, and consists of things such as insoles, splints, manipulation, or casting. Surgery is required much less frequently, and is reserved only for some of the severe types of flat foot that do not respond to conservative therapy.  Surgical Treatment Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot, meaning you will be on crutches for two months. The bottom line is: Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention. Prevention So how do you prevent plantar fasciitis? Factors which can be controlled include training progression, environmental factors, shoes, and strength and flexibility exercises. A useful guideline for a safe training progression is ?the 10% rule.? Limit increases in distance or intensity to 10% a week. For example, if a person is running 60 minutes at a session, 4 times a week, or 240 minutes, she or he can probably increase the running time to 264 minutes (240 + 10%), the following week if all else remains the same. Terrain is also an important factor in training. Running 30 minutes on hills is very different from running 30 minutes on flat surfaces in terms of the forces on the legs and feet. Work up gradually to increase your running time on hills. Also lean forward when running downhill. If you run on a banked or crowned surface, vary the direction you run in so you alternate which leg is higher and which leg is lower on the bank. If you know concrete or asphalt is causing you discomfort, try running on a cinder or composite track. If you are going on vacation and are not used to running on sand or grass, don?t spend your whole vacation doing it. Stretching Exercises Plantar Fasciitis stretches can be incorporated into a comprehensive treatment regime which may involve: ice, heel wedge support, taping, massage, muscle strengthening, orthotic inserts for shoes, topical anti inflammatory gel or oral medication and/or corticosteroid injections. If you suspect you may have Plantar Fasciitis seek accurate diagnosis and treatment from a health professional to ensure a correct diagnosis and reduce the likelihood of developing chronic foot pain. Treatment interventions may be provided by your Physical Therapist, Podiatrist and/or doctor. |
